McConnell Says Impeachment Accounts for Trump’s Coronavirus Failures



So, last weekend Trump pivoted toward keeping us on lockdown, in order to see whether we can hold down total deaths to somewhere in the neighborhood of 200,000—and to keep new outbreaks from spreading into rural red states during the summer and fall. Multiple sources say he finally listened to the scientists because he finally grasped the political implications of ignoring them.
Trump continues to lie like a rug, but his decision to turn on a dime on the social distancing issue has left many of his cultists in a confused psychological state. For example, will Jerry Falwell, Jr., having reopened Liberty University in what has aptly been called an act of right-wing performance art, now close it again? Will the governor of Oklahoma now stop telling people to to go out to restaurants? Will the governor of Florida make sure the beaches are closed?
Who can say? But let me recommend this incisive analysis of The Coronavirus and the Conservative Mind: The pandemic has put psychological theories of politics to a very interesting test.
The one thing that I have been saying that never came across particularly clearly in the way some people — and I’m not mentioning names — have expressed this: We are in the escalating phase of a very serious pandemic. That is a fact. We have got to realize that and to prepare and respond. It is not, as it were, under control.
Further to the topic of my last post, see Susan B. Glasser, The Trump O’Clock Follies: The President’s mendacious nightly press briefings on the coronavirus will go down in history for their monumental flimflammery:
During the Vietnam War, the United States had the Five O’Clock Follies, nightly briefings at which American military leaders claimed, citing a variety of bogus statistics, half-truths, and misleading reports from the front, to be winning a war that they were, in fact, losing. Richard Pyle, the Associated Press’s Saigon bureau chief, called the press conferences “the longest-playing tragicomedy in Southeast Asia’s theater of the absurd,” which, minus the “Southeast Asia” part, is not a bad description of the scene currently playing out each evening in the James S. Brady Press Briefing Room, in the White House. We now have the Trump Follies, the nightly briefings at which President Trump has lied and bragged, lamented and equivocated, about the global pandemicthat poses an existential threat to his Presidency. Just as the Vietnam briefings became a standard by which the erosion of government credibility could be measured then, historians of the future will consult the record of Trump’s mendacious, misleading press conferences as an example of a tragic failure of leadership at such a critical moment.
Emily Badger and Kevin Quealy, Red vs. Blue on Coronavirus Concern: The Gap Is Still Big but Closing
Charles Warzel, Trump Chooses Disaster as His Re-Election Strategy: It’s a massive bet that political polarization is a more powerful force than the virus’s body count.
Andrew Sullivan, America Is Trapped in Trump’s Blind Spot
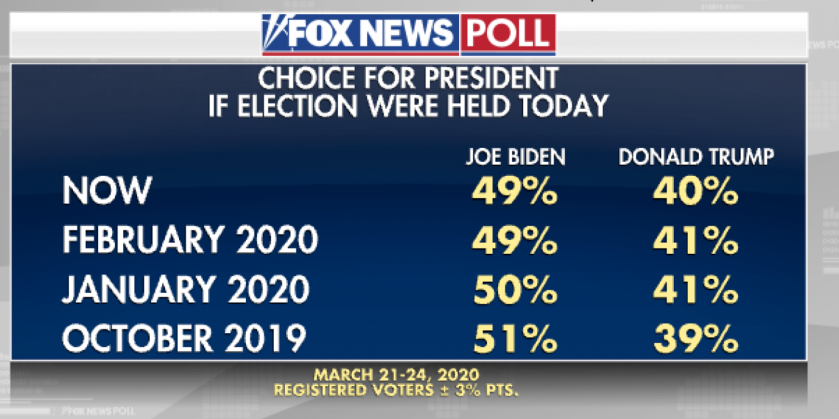
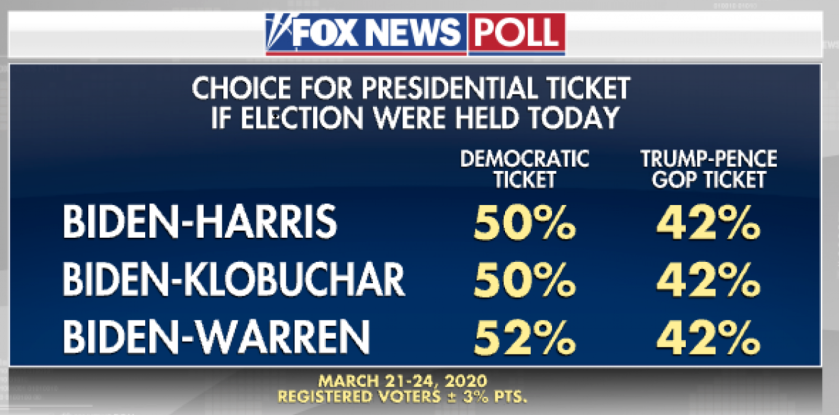
All the data in the last few days show that the Trump Bump in popularity is continuing. A number of generally reliable pundits have given a pollyannish spin on this development, and I hope they are right. My own view is that you can fool some of the people some of the time, and that Trump’s nightly coronavirus shit shows are currently fooling a few more people a little more of the time.
The question is what happens going forward. How many bodies will pile up, and where, and how will the Trump Base respond to his abdication of leadership? After all, they fell for Trump’s con and thought they were electing a strong leader. What they actually got was an authoritarian weakman.
Andrew Sullivan sees Trump’s behavior in this crisis as flowing directly from his mental deficiencies. Think of it this way. I barely passed elementary calculus. If you, nonetheless, insist that I plan the trajectory of your next missile launch, then you should bloody well not be surprised if the missile lands in the wrong place.
By contrast to Sullivan, Warzel presents Trump’s dastardly behavior during the crisis as a choice. But, I suppose that, in the end, it doesn’t matter whether Trump’s malfeasance results from irresistible impulse or from conscious choice. What matters is how his base reacts, as the bodies pile up and as the churches don’t reopen for Easter services.
So let me say three things about that. First of all, we don’t know the answer. Second, the material laid out in the Badger/Quealy piece is very informative, and generally hopeful.
Third, I rely not only on data and analysis but also on what my own gut tells me. I grew up among people who were racists then, who are still racists now, and who are Trump supporters. They have those characteristics in common, but there are lots of differences too. There are white trash bully boys, there are mild-mannered store clerks, and there are professors and doctors and nurses and lawyers.
What the data tell me, what common sense tells me, and what my gut tells me, is that there is a limit to their irrationality. And even, may I say, a limit to the irrationality of the white trash bully boys.
And so, on the day when Trump fires Dr. Fauci, what are these people going to say, and what are they going to do?

If, by chance, you do not know who the Reverend Ralph Drollinger is, then permit me to tell you. Rev. Drollinger is the spiritual leader of the White House Bible Study Group, which includes ten Cabinet members.
Recently, Rev. Drollinger applied his high theological wisdom to the question whether the coronavirus represents the wrath of God on America—a topic I addressed in my last post. His detailed taxonomy of the various forms of divine wrath may be found in an essay titled Is God Judging America Today?
Great theological minds, it is said, think alike. I am, accordingly, more than gratified to find that, after much hemming and hawing, zigging and zagging, toing and froing, Rev. Drollinger concludes, with me, that we are experiencing the form of divine wrath that comes from sowing the wind and reaping the whirlwind.
Regrettably, the reverend does not describe in any detail the nature of wind that we have sown, i.e., the exact source of the whirlwind we now reap. For that, you will have to turn to my theological analysis.
It is a well-known fact that God is in the business of micromanaging the universe. The thought is captured in this beautiful hymn:
Unfortunately, some professed Christians deny and revile one of God’s greatest gifts: our rational minds, and our ability to do scientific investigation. A New York Times op-ed captures the consequences of this grievous impiety: The Road to Coronavirus Hell Was Paved by Evangelicals: Trump’s response to the pandemic has been haunted by the science denialism of his ultraconservative religious allies.
If God micromanages the universe, it follows as the night the day that God micromanages who gets covid-19 and who doesn’t. Thus, as the Times op-ed notes, some pastors are keeping their churches open and packed on Sundays, confidently declaring that God will protect them.
And, by like token, on a larger scale, God has the power to micromanage which countries suffer the worse outbreaks and which do not. If, today, the United States is suffering the worst ravages of the pandemic, it must because God is especially angry at the United States.
Likewise, if God starts killing congregants at megachurches that defy the pandemic and stay open for business, it follows by ineluctable logic that God is angry at them.
And what, you may well ask, would be the reason for God’s anger at the United States, and His coming decimation of the megachurches?
There can be one reason, and one reason only: divine rage at the impious denial and refusal of His greatest gift, the gift of reason.
As one of my posse remarked yesterday, “Two paths diverged in a yellow wood, and America chose the psychopath.”
And now, ladies and germs, let us all rise for our closing hymn.


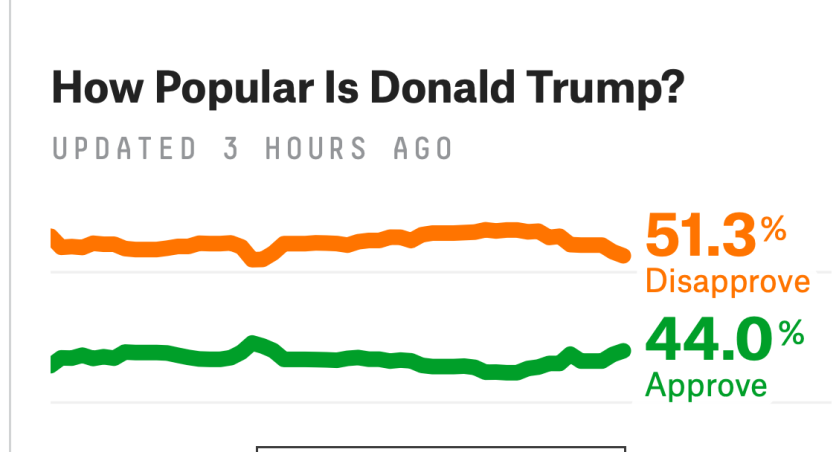
This afternoon, fivethirtyeight.com’s poll of polls shows a distinct uptick in Trump approval. Unbelievable. Meanwhile, Stanley Greenberg, a Democratic pollster, assures us that Americans’ Revulsion for Trump is Underappreciated: As Democrats fret about their own prospects, many fail to recognize the president’s fundamental weakness. Welcome news, provided It’s actually true.
Someone broke my crystal ball, so I’ll go on gut and logic. Pretty soon, Trump is going to order us back to work. (See Greg Sargent, A viral plea to let grandparents sacrifice themselves captures a truth about Trump.)
And that is when the shit will well and truly hit the fan.
I’m receiving lots of good questions from my last post, and have tried to answer all of them. I thought it might be helpful to post a few things so all of us can make informed decisions based on data wherever possible. This will be my last super-long post. Going forward, the bulk of the posts will be short and will provide links to a temporary site I set up on my lab website at: https://med.stanford.edu/utzlab/coronavirus-resource-page.html. This site also includes pdfs of primary publications containing the data. I am in the process of transitioning the website to the official Stanford Medicine site. Please note that everything in my list serve posts and website represent my personal interpretation of data and does not represent Stanford Medicine’s views. I don’t think anything I have written contradicts the CDC or Stanford, but if I learn that something I have written conflicts, I will post this.
Evidence-based advice on routine activities while we are sheltered in place. Effective shelter in place guidelines have already been shared in many posts and should be rigorously followed. The most common activities other than exercise that many of us still have to do are fueling cars, shopping for food, picking up medications, getting take out food, and delivering things to high-risk people. A paper was published in the New England Journal of Medicine (available from the above temporary site) that carefully studied how long the virus can survive on various surfaces. Data on key surfaces is below:
Copper – no viable COVID-19 after 4 hours
Cardboard – no viable COVID-19 after 24 hours
Stainless steel – no viable COVID-19 after 48 hours
Plastic – no viable COVID-19 after 72 hours
Not tested – glass, rubber, clothing, carpeting, tile, wood, stone, paper, and foods. No documented food transmission, cooked or uncooked, has been reported to my knowledge.
It is important to understand several things about these numbers:
Practical advice on how to use these data to make decisions when out in the community:
Thanks, and please don’t respond unless you have a specific question to cut down on email traffic. Feel free to forward this – but follow the rules our ListServe manager requested.
STAY HOME!
PJ Utz
Moreover, while she is inclined toward optimism by nature, I am afraid that Trump’s doctor impersonation is not helping matters for Pollyanna.
Washington Post, Fauci disputes Trump on available treatment drugs, says it’s about hope v. proof:
Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, was asked at the daily White House coronavirus news briefing about an hours-earlier tweet by Trump that claimed the FDA was working on a combination of an anti-malaria drug and an antibiotic that could treat the infection.
“I’m not totally sure what the president was referring to,” Fauci said …
Not everyone—including, apparently, some reporters—is aware of how drug regulation works. The FDA requires that drugs be (1) safe and (2) effective, and regulates the labeling and advertising of the drugs. Thus, if Drug X has not proved effective in treating histoplasmosis, then its label cannot indicate that it is effective for that use, it cannot be advertised for that use, and the drug company cannot lawfully urge doctors to prescribe it for that use.
BUT BUT BUT it is legal for doctors to prescribe drugs for “off-label use,” and this often happens, when there is some reason to believe a drug may be effective for a particular use and the circumstances are exigent, but the testing has not caught up with FDA standards.
All that said, Trump did not stay in a Holiday Inn Express last night, so I don’t trust him to play a doctor on TV and prescribe drugs for off-label use.